As you can see above, the province of Nova Scotia is now providing a graphical resprentation of the Covid-19 data. Further, the province has real laboratories, one of which processed an astounding 900 tests on Wednesday.
If journalists and lab technicians have the time, I think this is an accomplishment that derserves some coverage.
Turpin Laboratories, which is imaginary, will now find something else to do. Our staff are simply too exhausted to compete with the province.
Lastly, young whippersnappers take note: The province’s site has a breakdown Covid-19 cases by age group. You can no longer say you weren’t warned.
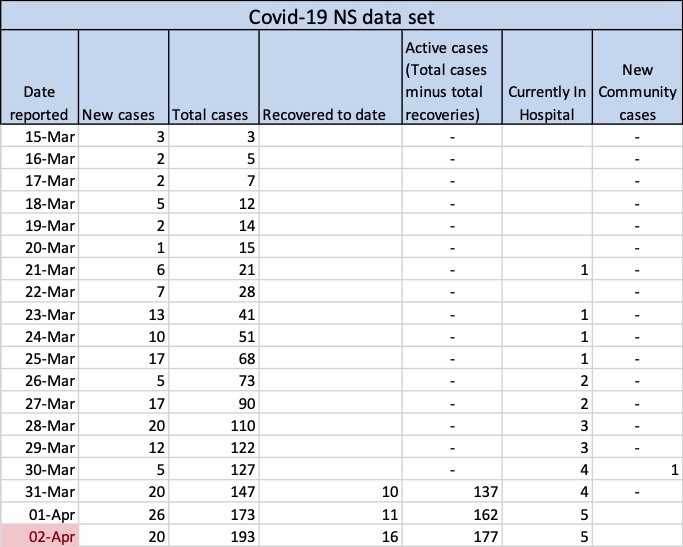
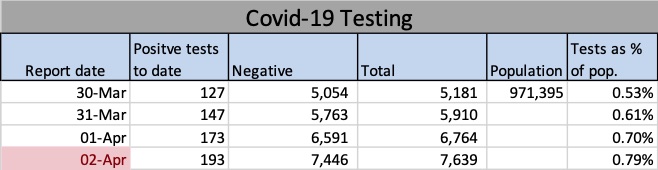
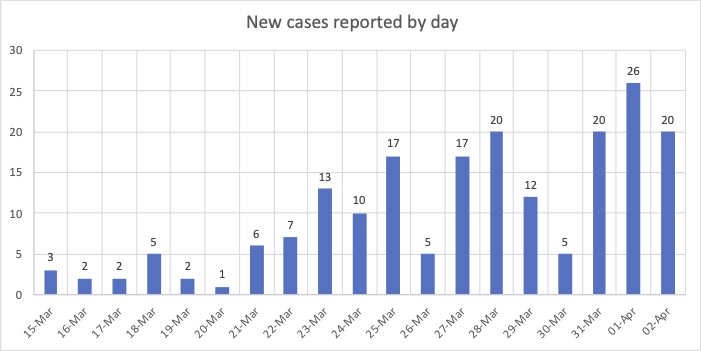
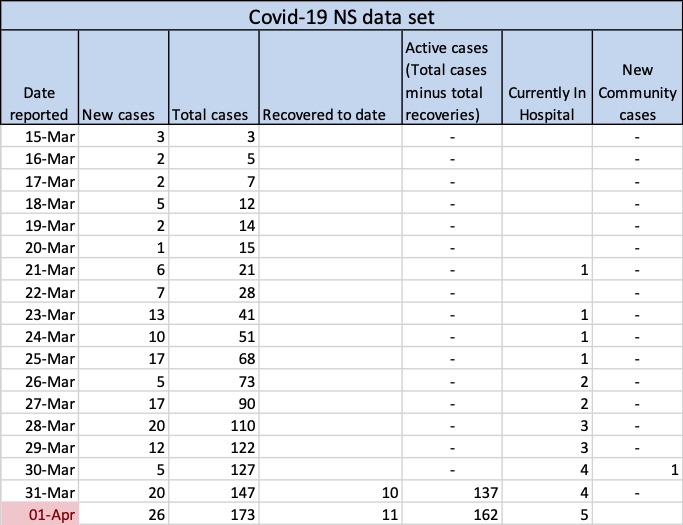
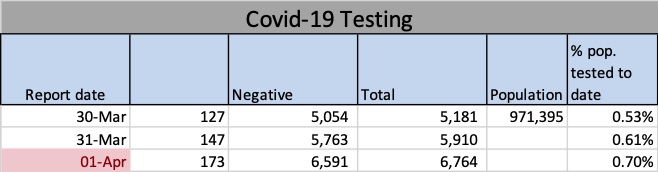
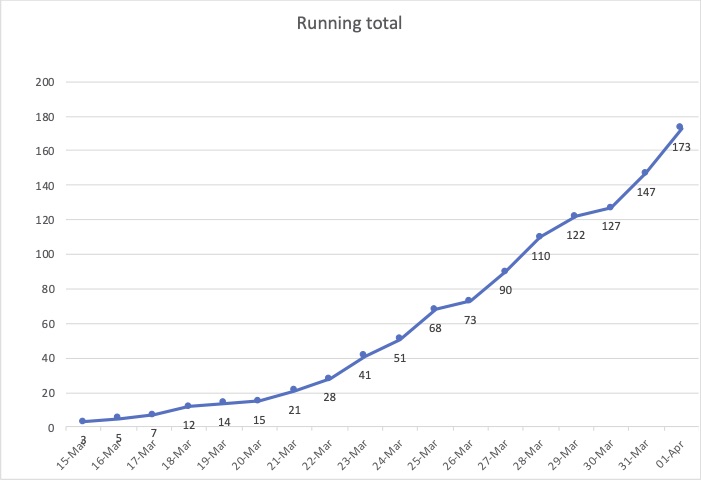
Above are the data used to create the charts and graphs you’ll find below. The cell highlighted in red shows when I last updated them.Above: “Positive cases to date” reflects confirmed cases of Covid-19 in Nova Scotia, e.g., 147 on March 31. Negative results and the total number of tests administered in the province are also shown. The rightmost cell shows the total for tests as a percentage of the population.The chart above (New cases reported by day) shows the number of Covid-19 cases reported each day by NS public health. For example, the first three cases were reported on March 15, two more were reported on March 16 and another two on March 17. The chart below (Running total) shows what happens when you add those number up. For example, the number corresponding to March 17 below is seven, the sum of March 15,16, and 17 above (3+2+2=7). You can find the news releases on the government’s searchable database at https://novascotia.ca/news/.The chart above is the result of summing all the available results as of date on the horizontal axis. The number 147 does not mean 147 cases were reported on March 31: rather, it’s the total of all 17 reports from March 15 to March 31, inclusive. As you can see on the bar chart, only 20 new cases were reported on March 31.
This post contains NS data on the Cover-19 outbreak here and will be updated regularly. You can see that as of April 1 a total of 173 cases had been reported. (Please note the name of this blog, Turpin Laboratories, was a tongue-in-cheek choice made during happier times. I am not a laboratory and possess no scientific expertise.) Everything below is presented for your reference only. Drawing conclusions from these data is is ill-advised unless you’re an expert. Further, you can see from the way the numbers jump around that predictions would be meaningless — especially, to paraphrase Yogi Berra, if they’re about future.
Above are the data used to create the charts and graphs you’ll find below. The cell highlighted in red shows when I last updated them.Above: “Positive cases to date” reflects confirmed cases of Covid-19 in Nova Scotia, e.g., 147 on March 31. Negative results and the total number of tests administered in the province are also shown. The rightmost cell shows the totals tests as a percentage of the population.The chart above (New cases reported by day) shows the number of Covid-19 cases reported each day by NS public health. For example, the first three cases were reported on March 15, two more were reported on March 16 and another two on March 17. The chart below (Running total) shows what happens when you add those number up. For example, the number corresponding to March 17 below is seven, the sum of March 15,16, and 17 above (3+2+2=7). You can find the news releases on the government’s searchable database at https://novascotia.ca/news/.The chart above is the result of summing all the available results as of date on the horizontal axis. The number 147 does not mean 147 cases were reported on March 31: rather, it’s the total of all 17 reports from March 15 to March 31, inclusive. As you can see on the bar chart, only 20 news cases were reported on March 31.
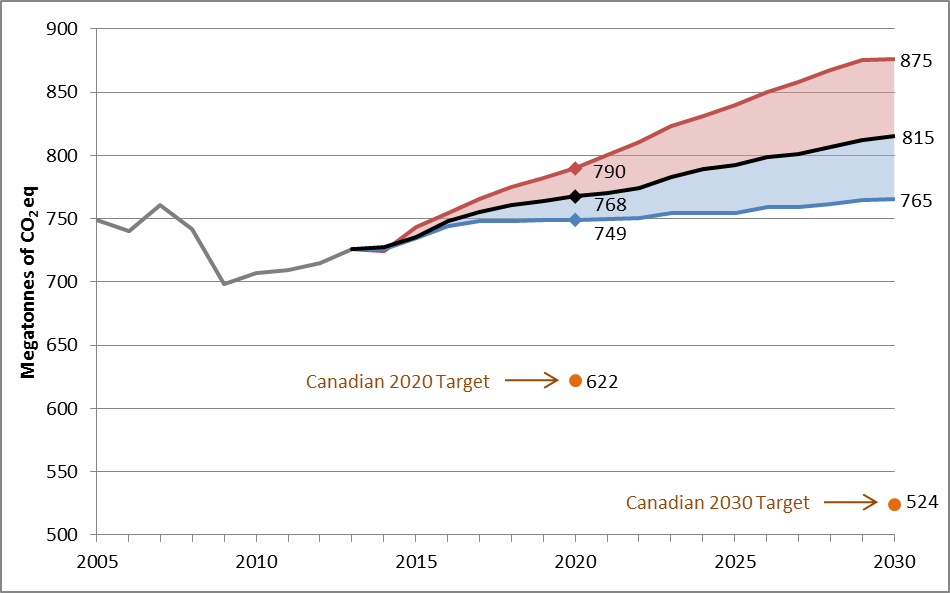
Propagandists for ExxonMobil were almost certainly a factor in Canada’s poor record of fighting climate change.
The figure shows that Canada’s greenhouse gas emissions projections under a “with current measures” scenario are projected to be 768 megatonnes (Mt) CO2 eq in 2020 and 815 Mt CO2 eq in 2030. It also shows the expected range of the same projections under different economic and energy price and production scenarios. For 2020, the expected range of emissions could be between 749 Mt and 790 Mt. For 2030, the expected range of emissions could be between 765 Mt and 875 Mt. It must be noted that these projections do not include contributions for the land use, land-use change and forestry sector (LULUCF), as analysis of alternative accounting approaches remains ongoing. (Graph by Environment Canada)
IT SEEMS there’s never a law around when you need one.
I’m thinking of climate criminals, people who undermined climate change science for decades when they knew it was valid and were well aware that ignoring it meant human catastrophe. They’re getting away with murder. (Climate criminals do not include the ignorant. Ignorance is not a crime.)
But what about people like Rex Tillerson, the former chief executive officer of ExxonMobil and U.S. secretary of state?
Exxon was the corporate Joseph Goebbels of the losing war against climate change, sowing confusion and doubt about climate science. Doubly damning, the company did so despite research, from its own scientists, going back to 1977 aboutthe reality and deadly implications of climate change.
Tillerson began his career with Exxon in 1975 and quickly rose to the company’s upper ranks. He cannot pretend he didn’t know about the vile propaganda his company was spreading or that he couldn’t have done something about it.
I like to think a Canadian criminal court could jail Tillerson under Section 219 of the Criminal Code:
Criminal negligence
219 (1) Every one is criminally negligent who
(a) in doing anything, or
(b) in omitting to do anything that it is his duty to do,
shows wanton or reckless disregard for the lives or safety of other persons. (Emphasis added.)
The maximum sentence when lives are lost is life in prison .
Former Exxon CEO and U.S. secretary of state Rex Tillerson (Wikipedia)
It’s reasonable to argue that Tillerson’s collaboration in a disinformation campaign against climate change science shows a “wanton disregard for the lives or safety of others”.
On the other hand, you could argue that investigating one of the world’s 10 largest companies is too much of an undertaking for our tiny country. However, much of the groundwork has already been done by U.S. states on behalf of Exxon shareholders. They’re arguing in civil court that shareholders weren’t properly advised of the threat to the value of their holdings posed by climate change.
Here, courtesy of the Pulitzer Prize-winning Inside Climate News is an overview of legal actions against Exxon in the U.S.
I’m certain the plaintiffs would gladly share their evidence against Exxon with Canadian investigators and I would like to see similar lawsuits here, but I’m far more concerned about the well-crafted public deception that undermined the fight against climate change.
Scientific Americansays “One thing is certain: in June 1988, when NASA scientist James Hansen told a congressional hearing that the planet was already warming, Exxon remained publicly convinced that the science was still controversial. Furthermore, experts agree that Exxon became a leader in campaigns of confusion. By 1989 the company had helped create the Global Climate Coalition (disbanded in 2002) to question the scientific basis for concern about climate change. It also helped to prevent the U.S. in 1998 from signing the international treaty, known as the Kyoto Protocol, to control greenhouse gases. Exxon’s tactic not only worked on the U.S. but also stopped other countries, such as China and India, from signing the treaty.” (Emphasis added.)
Remember, Exxon did this while possessing its own research validating climate change science.
So, I would like to see criminal charges under Section 219 and extradition requests to the U.S. for Tillerson and other Exxon executives.
But let’s not stop there. My guess is there are hundreds of equally guilty Canadians working for Exxon or other fossil fuel companies. As noted, the U.S. has done the groundwork, so let’s use it to hunt down our own climate criminals.
I understand that lawyers would probably shoot down this idea down because of some legal subtlety.
OK fine. Then we need a new law to instill palpable fear in Canada’s executive suites about degrading the environment. For example, executives inclined to secretly pollute so much as a trickling stream should be prepared for jail.
The environment is not an abstract concept: it’s our habitat. We are not trying to save the planet, which has survived climate change before; we are desperately trying to save ourselves.
People who get in the way belong behind bars. If our current laws can’t do the job, then let’s write new ones.
December is off to a good start for the Nova Scotia Health Authority.
This month it is able to report the first significant decline in the number of citizens who need a family doctor but cannot find one.
5,322 people reported they had found a family doctor and 3,738 registered with NSHA to get help in finding one.
That’s a net improvement of 1,584, the first decline since January. The final number is even better because, beginning this reporting period, NSHA can include results from the Patient Attachment Incentive Trust, which offers docs a one-time payment of $150 for each new patient they take on.
It began April 1 but the results were not counted until now, giving NSHA the benefit of eight months’ of incentives in a single entry.
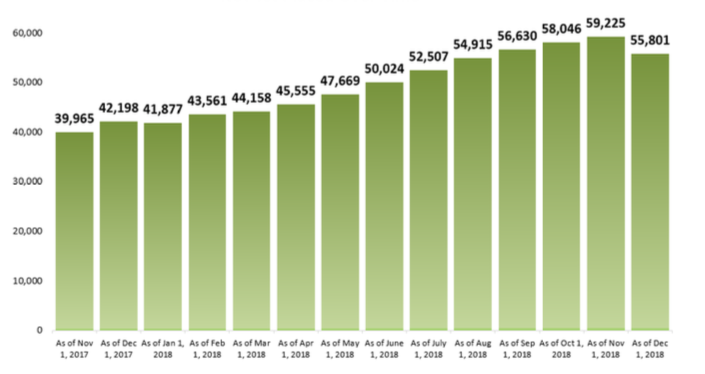
That means there are 55,801 doctor-less citizens as of December 1, down from 59,225 on November 1 (3,424). Whatever number you settle on, it’s a little bit of good news.
NSHA graph shows number of doctor-less Nova Scotians, based on its registry. The December 1 number shows an encouraging improvement. It’s accurate, but a little misleading.
Architect’s rendering of the new entrance to Dartmouth General, which opened today, December 10. The official opening is tomorrow, December 11.
And there is more good news at Dartmouth General. The official opening of its new entrance, which faces Acadia Street, happens tomorrow, Dec. 10.
In your correspondent’s view, the “official” opening of a door is a good idea when it’s part of a $140-million renovation because it’s a chance to remind the public this important project is well underway, which makes it harder for governments to stop it.
I say this with the lonely saga of DGH’s ghost floor in mind. It’s the building’s fifth floor, built circa 1988 but left empty until now.
Citizens may recall that during the ghost floor’s big sleep, emergency departments on both sides of Halifax Harbour were practising hallway medicine because there were no beds for emergency patients once they had been stabilized.
This will continue until the construction, finally underway, of the ghostly fifth floor is complete. But it’s galling to know that additional capacity has been available —on the ghost floor— for the last 30 years. It’s the kind of thing that makes voters cynical. Preventing hallway medicine is the responsibility of elected officials and all three political parties have dropped the ball at one time or another.
But enough negativity. The DGH project is itself a part of the much larger “QEII New Generation” project that will replace the VG, Centennial and Dickson buildings in Halifax.
NSHA’s Victoria van Hemert, who is overseeing the whole thing, says the changes at DGH will have a huge impact on the community.
“The big benefit is capacity,” she says. “It means services will be closer to people’s homes.”
Here are some of the other benefits:
48 new beds, some of which will accommodate morbidly obese patients
Renovations are finished on the third and fourth floors.
Eight new operating rooms (replacing four existing ones), which will increase surgical capacity by 3,500 operations per year.
Two of the new O.R.’S will be high-volume facilities dedicated to orthopaedic surgery, making DGH a key focus for those procedures.
Patient rooms will be spacious and offer a view of the outside wherever possible. They will be single-occupancy where feasible. Both features have been proven to speed recovery, reduce relapses and promote infection control.
Some rooms will have two patients, but that’s the maximum. There will be no four-bed wards.
Outpatient services capacity (procedures not requiring overnight stays) will double.
A three-storey addition is under construction and planned for completion next summer. It will house the new O.R.s, a new ambulatory care clinic (ongoing treatments not requiring an overnight stay, such as dialysis), and an endoscopy centre.
The entire project is expected to be finished by late 2021, which pretty much eliminates the possibility of progress being suspended by an election, as it did in 2009 and arguably 2013. This time Premier Stephen McNeil’s government seems to have the bit firmly in its teeth and technically has until 2022 to drop the writ.
Nonetheless, we should keep a sharp eye in the Halifax Infirmary redevelopment, which is ambitious, critical and expensive. Completion might come in 2024-25, which is a long way away in political terms.
NSHA has been refreshingly open about the doctor shortage and the hospital reconstruction. I hope they keep it up and even go further. Believe it or not, open government brings results.
CORRECTION: Earlier, I wrongly reported the fourth floor of Dartmouth General Hospital would be used for administration. It will continue to be an inpatient floor.
Predictably, the number of Nova Scotians in need of a family doctor hit a new high as of Nov. 1.
On the bright side, it’s “only” 1,179 more than the month before, and it’s the fourth number in a row suggesting some kind of moderating trend. So, fingers crossed, eh?
On the dark side, our 59,225 doctor-less citizens may lose access to a much-needed painkiller next year.
Health Canada is proposing to make low-dose codeine products available by prescription-only. This would include Tylenol No. 1, which is an alternative for people who cannot tolerate a class of common painkillers called NSAIDs. It includes Aspirin, Ibuprofen, Alleve and many others.
I’m not saying Tylenol No.1 is risk-free. Regular Tylenol (and its generic versions) contains acetaminophen, which by itself can have serious side-effects when misused, but is safe when guidelines are followed.
However, Tylenol No. 1 also contains codeine and caffeine, which are intended to boost the pain relief. Codeine is an opioid which, given the current paranoia over anything with that name, explains what’s going on here.
Health Canada has a stout defence of its proposal and I lack the science to debate the issue with them.
But I will say that even retail drugs can have unwanted side effects. The misuse of Aspirin and its cousins, for example, can cause stomach ulcers. The question is whether the benefits of a drug outweigh the risks.
If you have chronic pain, you might be willing to risk a lot for relief. (On the flip side, I know someone whose death likely began with a refusal to request opioids for severe pain.)
And I note Canadians take about 600 million doses per year of Tylenol No. 1, which pro-rates to about 15 million doses in Nova Scotia, the equivalent of 300,000 bottles containing 50 tablets. I don’t know how many prescriptions that will require, but the calculation starts at 300,000.
Whatever the final number is, it’s bound to be a burden for family doctors, some of whom have already endured oppressive and unnecessary prying by authorities waging a war on opioids. Nonetheless, a doctor I know supports the management of opioids even in small doses, but feels other types of painkillers should be made more accessible and less expensive. Interestingly, this doctor suggests including opioids among the drugs pharmacists are permitted to prescribe.
And that brings us to the biggest problem here: if Health Canada makes this change, how will you get Tylenol No. 1 if you don’t have a family doctor?
How many of our 59,225 doctor-less citizens will have go the infamous “street” for their pain relief? These folks are about six per cent of the province which, using my seat-of-the-pants calculation, equates to a potential market of about 18,000 bottles.
So that could be new biz for “the street” and its dangerous, unregulated products. That’s a lot of risk. I wonder if the benefits are worth it.
But I’m no expert. To quote the Great Ignoramus, I’m just sayin’, that’s all.
The $2-billion cost of revitalizing Nova Scotia’s most important medical centre, and the debate over the public-private-partnership (P3) approach to building it, have obscured a much more interesting feature of the project.
Far from the decentralization discussed just two years ago, it will create a health care powerhouse at the Halifax Infirmary site.
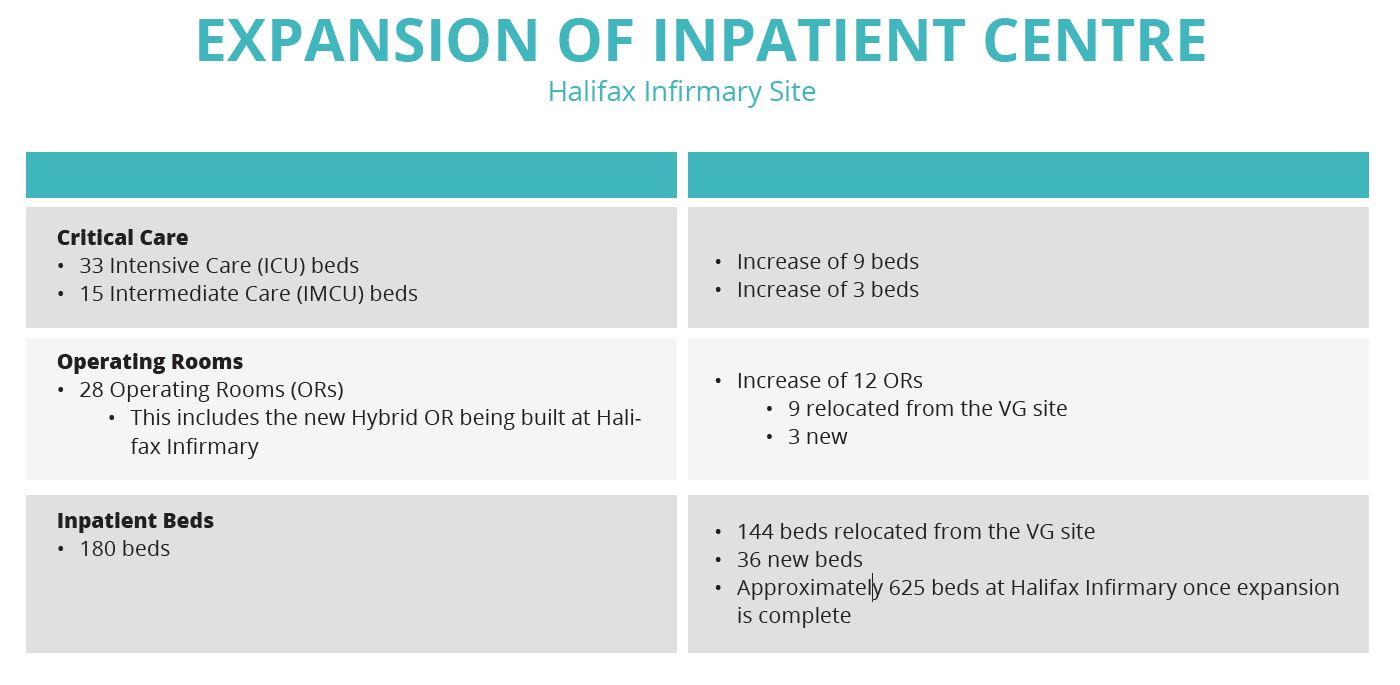
According to the Nova Scotia Health Authority, when the dust has settled in the middle of the next decade, the HI site will comprise 625 inpatient beds, 28 operating rooms, 33 intensive care beds and 15 intermediate care beds.
Increases are net, reflecting new facilities and transfers from the VG site. (Courtesy NSHA)
I know I should lower my expectations here. After all, the effort to bring the so-called Victoria General campus up to standard has been driven solely by hot air for at least 20 years. But the politically risky decision to make it a P3 build tells me Stephen McNeil’s government means business.
The VG campus, notwithstanding its disgraceful buildings, is supposed to be the centre of excellence for medicine in the Maritimes. We need to take note of what’s going to replace it.
For starters, the Infirmary parkade will be demolished and rebuilt underground, with a new inpatient building sitting on top.
The existing emergency department will remain where it is, but will be flanked by three new buildings dedicated to a research and learning centre, cancer care, and ambulatory care.
As late as April of this year, the plan was to retaincancer care at the Victoria General site, but planners decided patient health would be better served if the centre was part of the HI site. In part, it will permit views of the outdoors, communal space, gardens and natural materials designed to make cancer patients more at ease. It will also promote team care.
Whatever the decision, it will gobble up the communal vegetable garden occupying the site of the former QEII High School. But we don’t yet know whether the cancer care centre will occupy the garden site or the former CBC building on Bell Road. Planners will complete a study of patient flow before making that call. (See illustrations.)
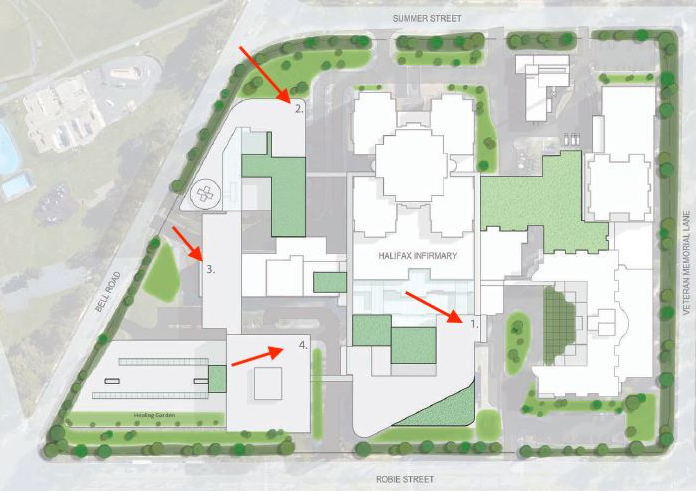
This concept illustration shows an area bounded by Robie St. at the bottom, then, moving clockwise, Bell Road, Summer Street and Veterans’ Memorial Lane. Arrows point to numbers on key buildings: 1-new inpatient building; 2-outpatient building; 3-learning and research centre; 4-cancer care building.
In sum, the site will have four new buildings: cancer care, ambulatory (outpatient), a research and learning centre, and an additional inpatient building. Dartmouth General is already undergoing an extensive remake that includes
In this concept, the locations of cancer care (4) and outpatient (2) have been swapped. Patient flow will be the key to the decision. In either case, the community garden will have to go. (Courtesy NSHA)
a new tower, and the rural-friendly community outpatient centre at Bayers Lake is going ahead.
So that’s a total of six new buildings.
A team approach to care is seen as one of the benefits of the new campus. For example, people with cancer often have other illnesses and will benefit when specialists can work along-side cancer-care providers.
The focus on patient comfort will extend to the 180 new inpatient units, 80 per cent of which will be single occupancy. This, as well as good views of the outdoors wherever possible, has been found to pay for itself in shorter stays and fewer returns to care. The remaining rooms will be similar but with a maximum of two patients and no sharing of bathrooms.
Victoria van Hemert, who heads the project, told your incredulous correspondent (who prefers to lick his wounds in remote caves) that some people actually heal better in a social setting.
As noted, the parkade on Robie will go underground with the additional inpatient building on top. Underground parking lots will also be constructed beneath the cancer care and outpatient buildings.
Interestingly, the net increase in “regular” inpatient beds on the Peninsula is just 36. But van Hemert, who has a number of successful hospital projects on her CV, says it’s the right number:
“This outcome was objectively derived based on programs and services, demographics (including age), technological changes, and more day surgeries. Epidemiologists were a part of the calculation. And then we looked ahead 20 years.”
Intensive care beds will go up by nine to 33; intermediate care will rise by three to 15.
There is some capacity to scale up the emergency department, but planners are counting on three things to ease the current overcrowding:
Expanded outpatient services (mastectomies, for example, can now be done on an outpatient basis);
Faster transfers of emergency patients to continuing care (home care);
Faster access to long-term care (e.g. nursing homes).
“More timely discharge of inpatients to Continuing Care and long-term care services will assist with improving flow of patients from the Emergency Department to inpatient units,” Nicole Brooks de Gier, community relations advisor for the project, said in an email.
That’s an understatement. Your correspondent has spent the night with family members in an emergency room on three occasions, once for 36 hours. The beds are actually gurneys, which are narrow and uncomfortable, and it can he hard to get help from staff because they are busy with, well, other emergencies.
In each case, the explanation was the lack of a hospital bed for my family member. Too many were already occupied by patients who belonged in a home or continuing care.
This is surely expensive, but it’s also hard on staff morale. “We’re trained and equipped for emergency medicine,” an exhausted emergency nurse told me one night. “Our job is to treat patients and send them home, or get them ready for admission to inpatient care. (Your relative) is not getting the right care here.”
Given the net increase in regular inpatient beds, it seems this $2-billion project has a lot riding on care given outside a hospital.
NOTES:
Part of the project is a new operating room at Hants Community Hospital. It’s completed and expected to handle 800 surgeries per year;
NSHA will own the buildings and deliver services
To come:
Dartmouth General expansion (ghost floor comes back to life)
As of the first of this month 58,046 (6.3%) Nova Scotians were in search of doctor. That’s an increase of about one-tenth of a percentage point, or 1,416 people.
On the upside, it’s far better than the increase recorded on July 1 which, as they say on TV, was a “whopping” 2,483. Since then, the monthly increase has been declining steadily, so maybe that’s good news (hard to say, as I have never been “whopped”.)
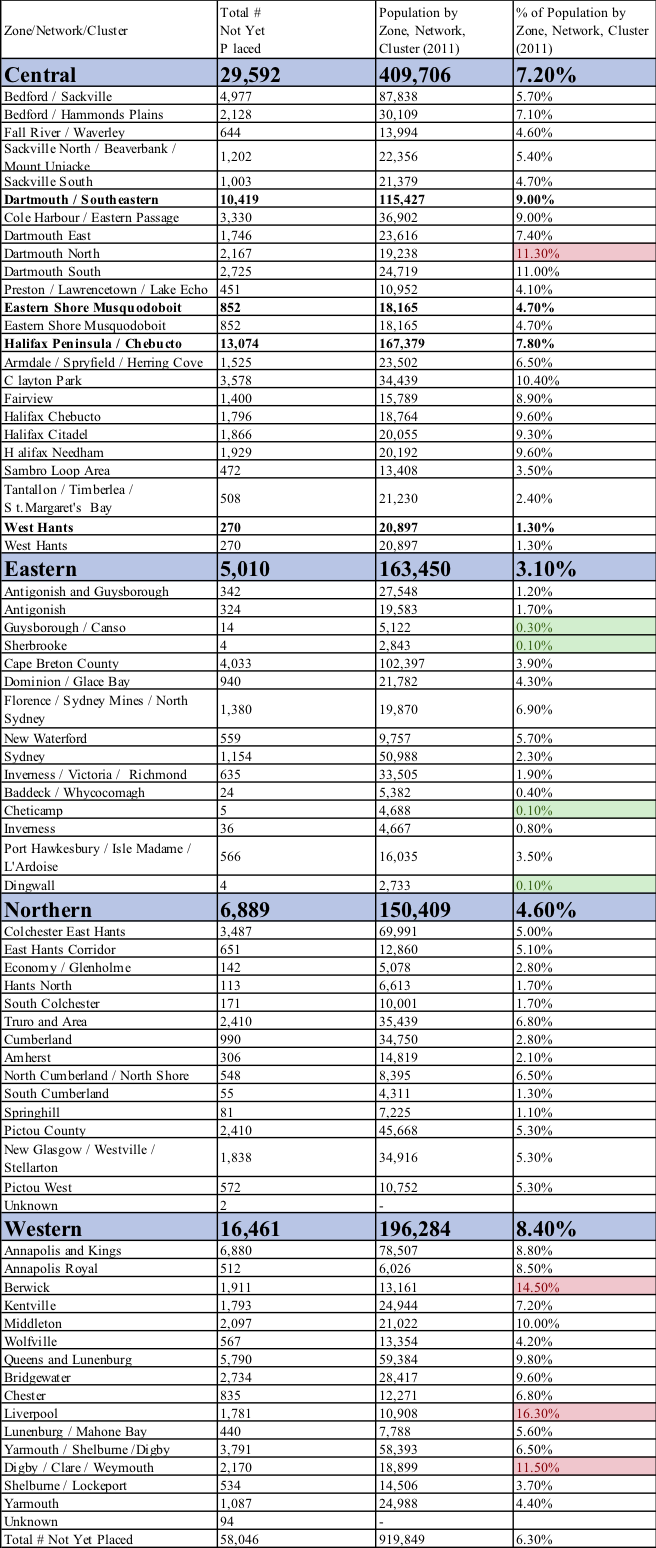
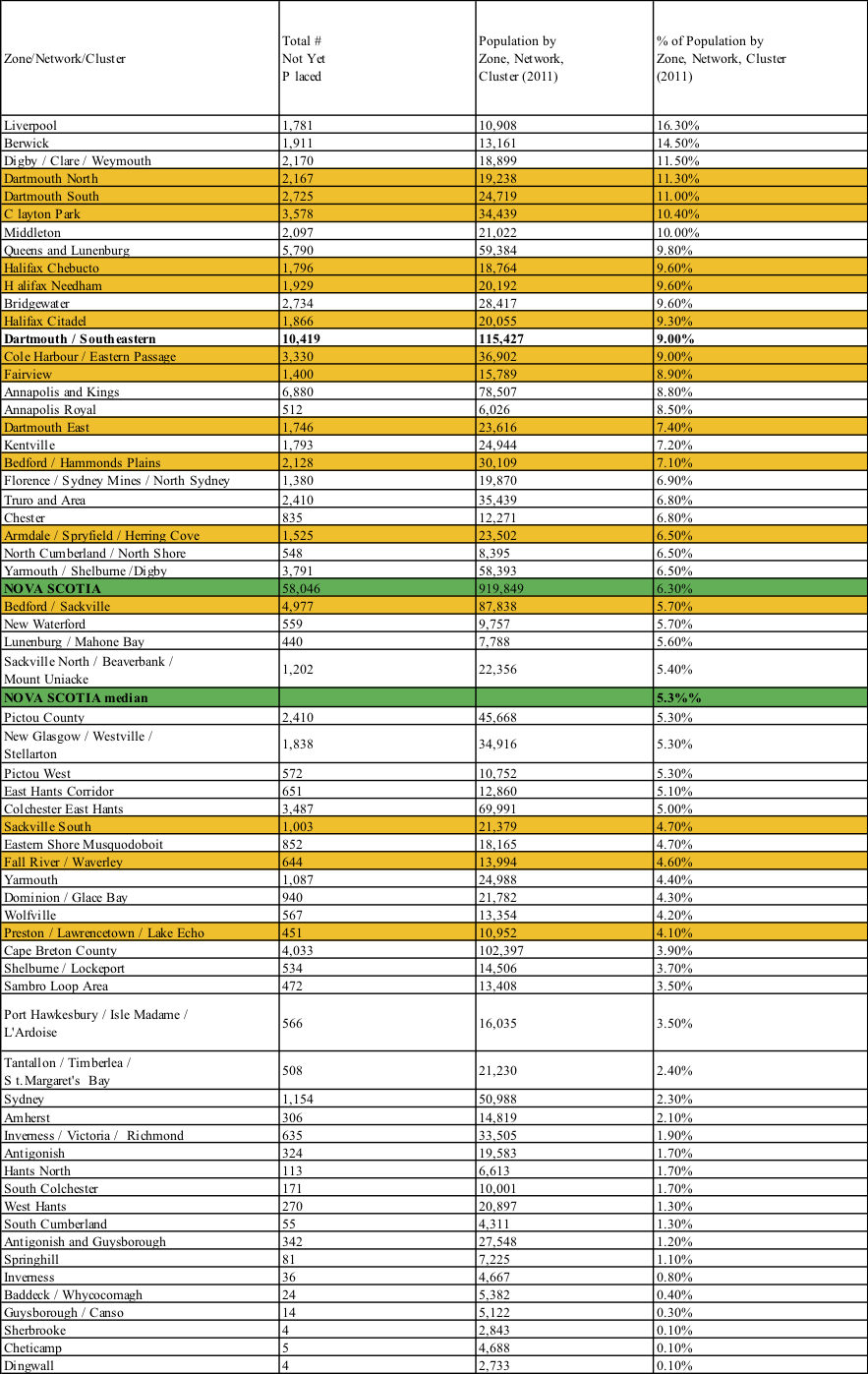
The data come from the Nova Scotia Health Authority, which has been notably open about the doctor shortage. Further, the October report contains new details offering a pretty good idea of the situation where you live, based on the percentage of people there without doctors.
In the first table below, I’ve highlighted the four best performers in green, and the worst in red. The Eastern Zone has all the best — four areas where there is effectively no doctor shortage, in my view.
Liverpool is in dire straits, with 16.3% of the population (1,781 people) needing but unable to find a doctor.
As usual, about half the people without doctors (29,469) live in Metro Halifax. That’s 7.7% of the city vs. 6.3% for the province. At the bottom of this post is a Halifax-centric table sorted from the highest percentage of people without doctors to the lowest. I’ve used a seasonal orange colour to illustrate the local problem, about which our councillors and MLAs don’t seem to care.
Highlighted table from NSHA
Halifax-centric table
This table is sorted from the highest percentage of people without doctors to the lowest. I’ve used a seasonal orange colour to illustrate the local problem, about which our councillors and MLAs don’t seem to care.
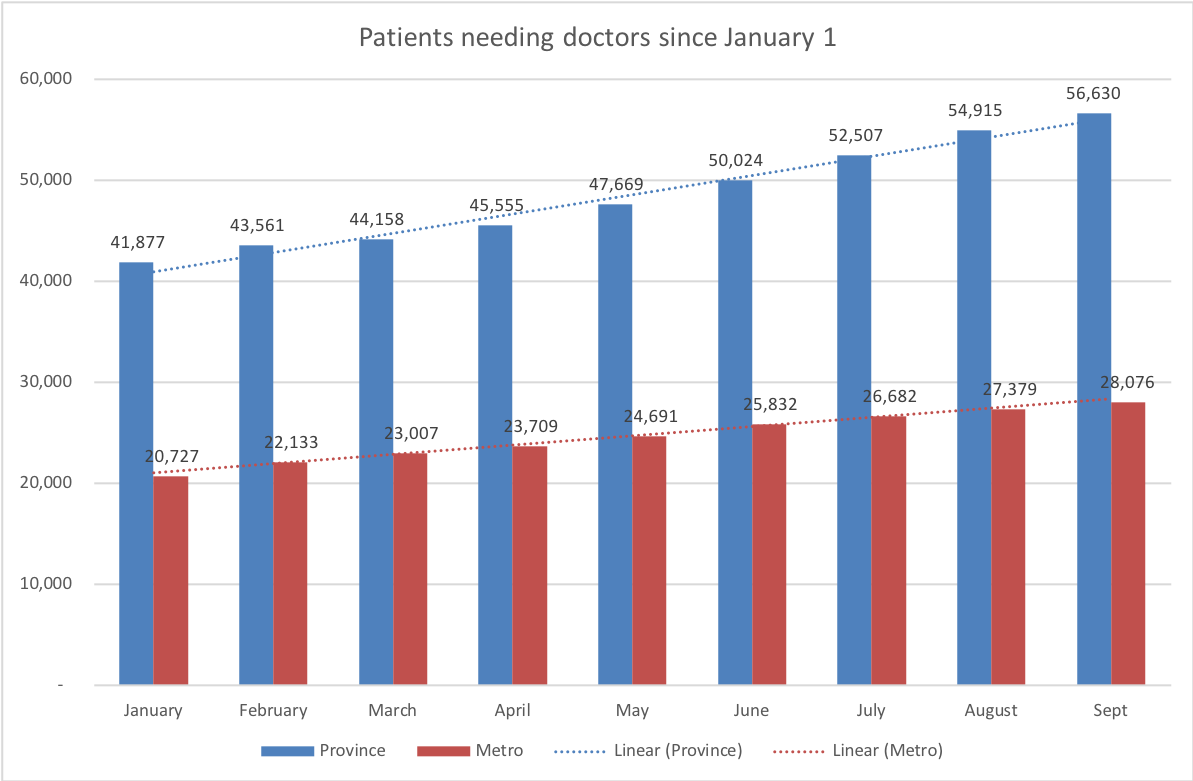
The past nine months show an almost linear growth of Nova Scotians wanting, but unable to find, a family physician. The current rate is 6.2 per cent of the population, up from 4.6 per cent in January. It represents another 14,753 people looking for a doctor for a total of 56,630. On the other hand, NSHA does its calculation based on the number of people who have registered with its Need a Family Practice Registry. It’s possible greater awareness of the registry is driving the numbers up. As usual, metro Halifax represents about half the problem. Source: Need a Family Practice Registry Monthly Report – September 2018
Steady increase since January
56,630 now seeking doctors
Two key players depart
Is good policy to blame?
TWO OF THE key players in the Nova Scotia Health Authority’s physician recruitment efforts have left the building in the past few days.
No doubt the alarming record of the past nine months is part of the reason (see chart above).
The health authority bases its numbers of the count of doctor-less people signed on to its Need a Family Practice Registry, something it strongly encourages. This makes sense because it’s realistic — you can be sure someone who’s taken the trouble to register truly needs a doctor. By contrast, surveys will count people who shouldn’t be counted: those who don’t want a family doctor but still, truthfully, say “no” when asked if they have one. That could be why Statistics Canada always reports a higher number than NSHA.
Put another way, the steady increase in the number of people needing doctors may be a reflection of a steady increase in awareness of the registration service. Can this be an example of sound policy being bad office politics?
We’re still losing ground to the physician shortage,
HRM still watching from the sidelines
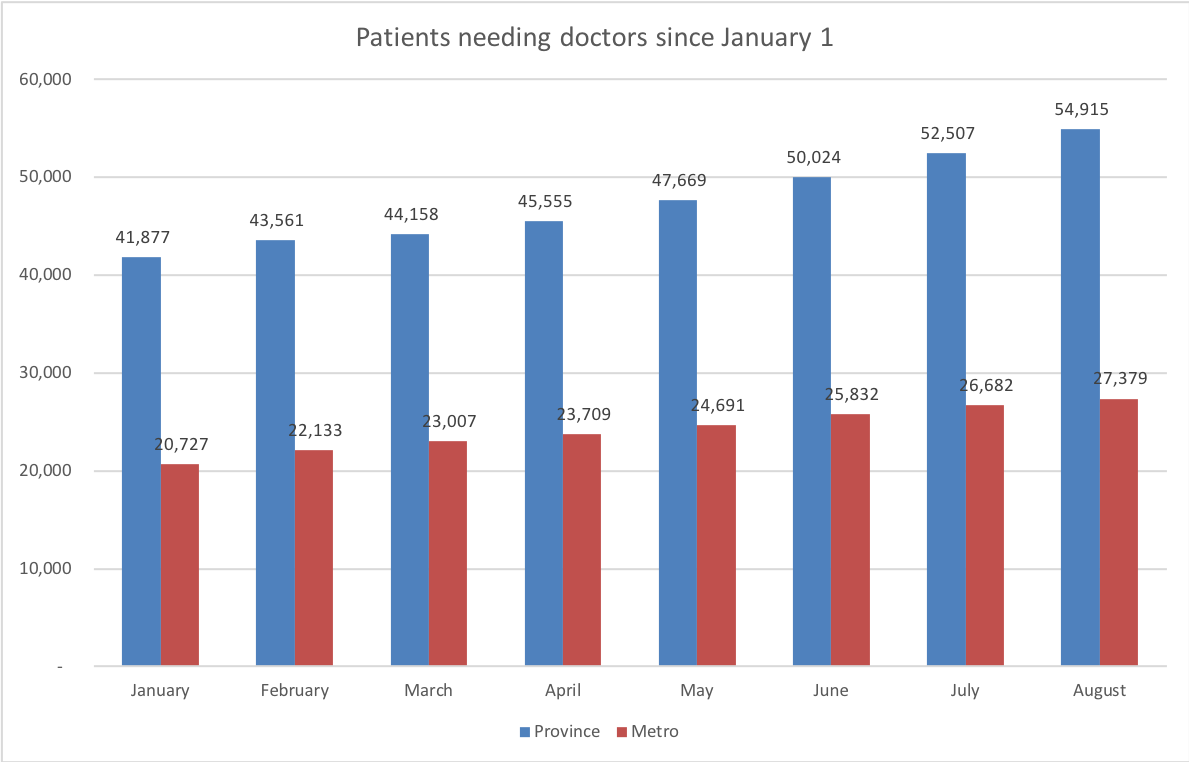
On the one hand, the Nova Scotia Health Authority’s latest stats on patients without doctors are nothing new — just another increase of a few per cent from the previous month.
On the other hand, it’s like compound interest on credit card debt. Everything seems OK until one day you’re in too deep. And so we’ve gone from 41,877 people needing a family doctor in January to 54,915 today. That’s six per cent of the population. By way of perspective, most of us would be thrilled with a six per cent return on our savings. In pre-election polls, six per cent can mean a lock on victory.
But the bad news doesn’t seem to be for lack of effort from government, which has brought in two new programs since January and made an important improvement to a third.
On the face of it, we seem to have our act together.
Since February, NS Immigration has operated a “physician stream” under the provincial immigrant nominee program.
In April, the Department of Health and Wellness launched the Patient Attachment Incentive Trust. It offers physicians a one-time incentive of $150 per head to take on additional patients. The trust brought 7,536 people in from the cold since it began in April. That’s a clear success. (But, alas, during that same period the net tally of people seeking doctors grew by 9,360.)
DHW continues to offer tuition relief, bursaries, debt assistance and a site-visit program. And these incentives now put Halifax on an equal footing with the rest of the province.
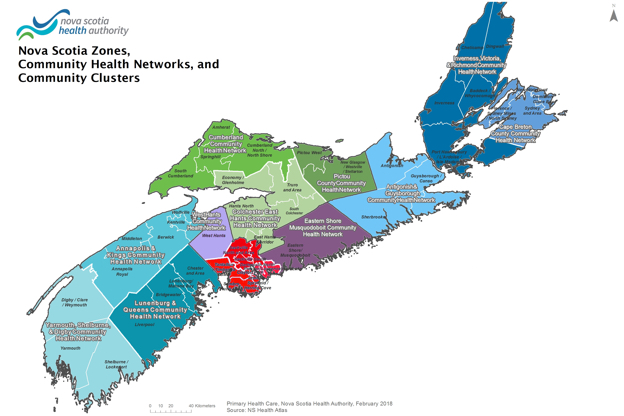
Area in red is “Metro Halifax”
All this makes it easier for recruiters working for the health authority and the IWK Health Centre. Let’s hope the effort starts paying off.
While we’re discussing effort, I note Metro Halifax (see map) consistently represents half of the provincial shortage, so it would be nice to see HRM contribute. Queens has an attractive website aimed at physician recruitment. Why not Halifax?
The growth in the number of Nova Scotians seeking but unable to find doctors climbed in June at a rate of 4.7%, or 2,483, which is in line with previous reporting periods.
Metro Halifax (the “health networks” of Bedford, Dartmouth South, Halifax and Chebucto Peninsulas) continues to be the locus of the worst problem, with 26,682 people seeking doctors (about 51% of the provincial total). Metro’s total is up 850.
The Central Zone (all of HRM) continues to represent about 54% of the problem.
In terms of raw numbers, the biggest change was in the Queens and Lunenburg health network, with 447 more people seeking doctors. In percentage terms, West Hants was hardest hit with increase of 27%.
The most dramatic improvement was in Inverness/Victoria/Richmond, where those needing doctors shrank by 17%, or 209 people.