Updated March 9, 2020
The $2-billion cost of revitalizing Nova Scotia’s most important medical centre, and the debate over the public-private-partnership (P3) approach to building it, have obscured a much more interesting feature of the project.
Far from the decentralization discussed just two years ago, it will create a health care powerhouse at the Halifax Infirmary site.
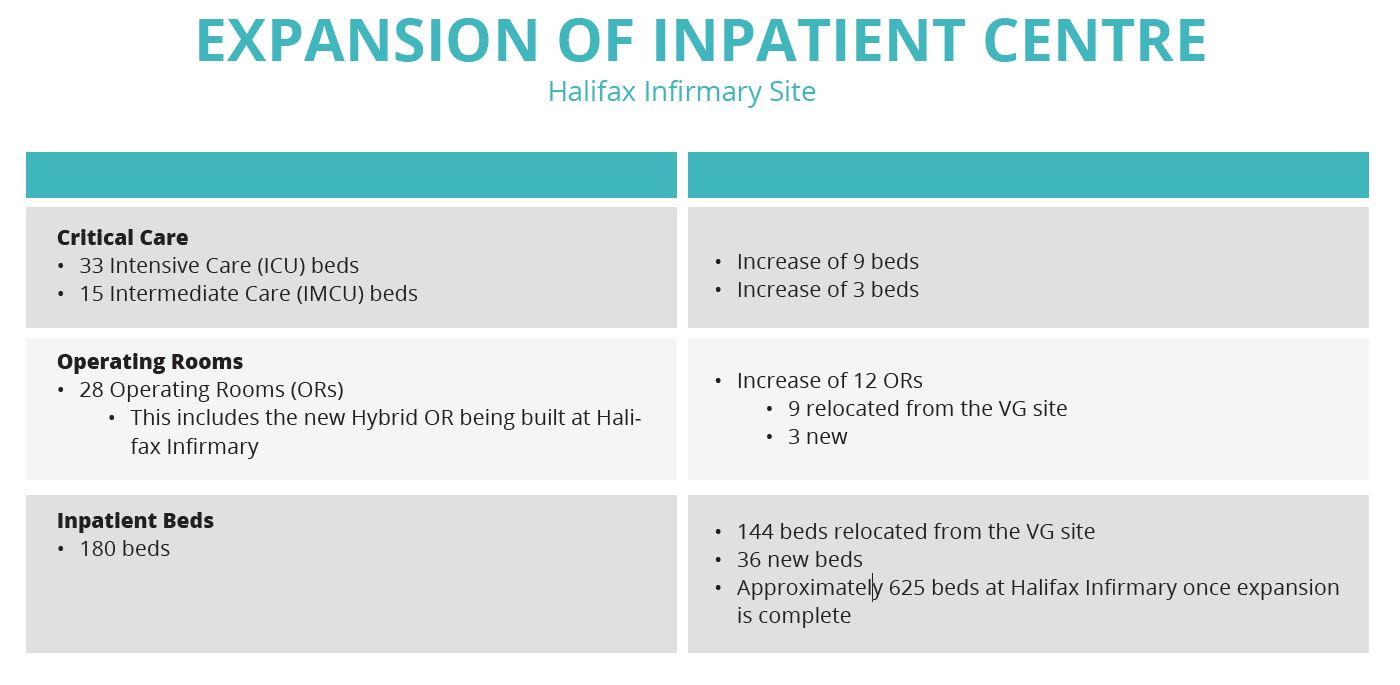
According to the Nova Scotia Health Authority, when the dust has settled in the middle of the next decade, the HI site will comprise 625 inpatient beds, 28 operating rooms, 33 intensive care beds and 15 intermediate care beds.
I know I should lower my expectations here. After all, the effort to bring the so-called Victoria General campus up to standard has been driven solely by hot air for at least 20 years. But the politically risky decision to make it a P3 build tells me Stephen McNeil’s government means business.
The VG campus, notwithstanding its disgraceful buildings, is supposed to be the centre of excellence for medicine in the Maritimes. We need to take note of what’s going to replace it.
For starters, the Infirmary parkade will be demolished and rebuilt underground, with a new inpatient building sitting on top.
The existing emergency department will remain where it is, but will be flanked by three new buildings dedicated to a research and learning centre, cancer care, and ambulatory care.
As late as April of this year, the plan was to retain cancer care at the Victoria General site, but planners decided patient health would be better served if the centre was part of the HI site. In part, it will permit views of the outdoors, communal space, gardens and natural materials designed to make cancer patients more at ease. It will also promote team care.
Whatever the decision, it will gobble up the communal vegetable garden occupying the site of the former QEII High School. But we don’t yet know whether the cancer care centre will occupy the garden site or the former CBC building on Bell Road. Planners will complete a study of patient flow before making that call. (See illustrations.)
In sum, the site will have four new buildings: cancer care, ambulatory (outpatient), a research and learning centre, and an additional inpatient building. Dartmouth General is already undergoing an extensive remake that includes
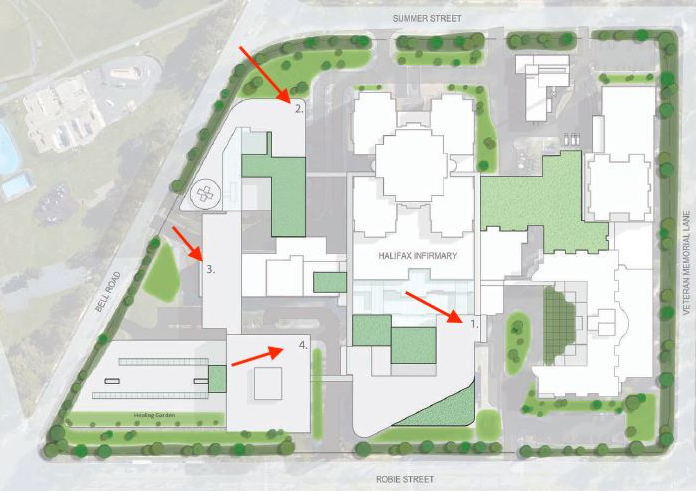
a new tower, and the rural-friendly community outpatient centre at Bayers Lake is going ahead.
So that’s a total of six new buildings.
A team approach to care is seen as one of the benefits of the new campus. For example, people with cancer often have other illnesses and will benefit when specialists can work along-side cancer-care providers.
The focus on patient comfort will extend to the 180 new inpatient units, 80 per cent of which will be single occupancy. This, as well as good views of the outdoors wherever possible, has been found to pay for itself in shorter stays and fewer returns to care. The remaining rooms will be similar but with a maximum of two patients and no sharing of bathrooms.
Victoria van Hemert, who heads the project, told your incredulous correspondent (who prefers to lick his wounds in remote caves) that some people actually heal better in a social setting.
As noted, the parkade on Robie will go underground with the additional inpatient building on top. Underground parking lots will also be constructed beneath the cancer care and outpatient buildings.
Interestingly, the net increase in “regular” inpatient beds on the Peninsula is just 36. But van Hemert, who has a number of successful hospital projects on her CV, says it’s the right number:
“This outcome was objectively derived based on programs and services, demographics (including age), technological changes, and more day surgeries. Epidemiologists were a part of the calculation. And then we looked ahead 20 years.”
Intensive care beds will go up by nine to 33; intermediate care will rise by three to 15.
There is some capacity to scale up the emergency department, but planners are counting on three things to ease the current overcrowding:
- Expanded outpatient services (mastectomies, for example, can now be done on an outpatient basis);
- Faster transfers of emergency patients to continuing care (home care);
- Faster access to long-term care (e.g. nursing homes).
“More timely discharge of inpatients to Continuing Care and long-term care services will assist with improving flow of patients from the Emergency Department to inpatient units,” Nicole Brooks de Gier, community relations advisor for the project, said in an email.
That’s an understatement. Your correspondent has spent the night with family members in an emergency room on three occasions, once for 36 hours. The beds are actually gurneys, which are narrow and uncomfortable, and it can he hard to get help from staff because they are busy with, well, other emergencies.
In each case, the explanation was the lack of a hospital bed for my family member. Too many were already occupied by patients who belonged in a home or continuing care.
This is surely expensive, but it’s also hard on staff morale. “We’re trained and equipped for emergency medicine,” an exhausted emergency nurse told me one night. “Our job is to treat patients and send them home, or get them ready for admission to inpatient care. (Your relative) is not getting the right care here.”
Given the net increase in regular inpatient beds, it seems this $2-billion project has a lot riding on care given outside a hospital.
NOTES:
- Part of the project is a new operating room at Hants Community Hospital. It’s completed and expected to handle 800 surgeries per year;
- NSHA will own the buildings and deliver services
To come:
- Dartmouth General expansion (ghost floor comes back to life)
- Continuing care and long-term care
- Bayers Lake outpatient centre
- Short rant in favour of P3 model
-30-

One thought on “Crucial transformation coming to Halifax Infirmary site”