- Propagandists for ExxonMobil were almost certainly a factor in Canada’s poor record of fighting climate change.
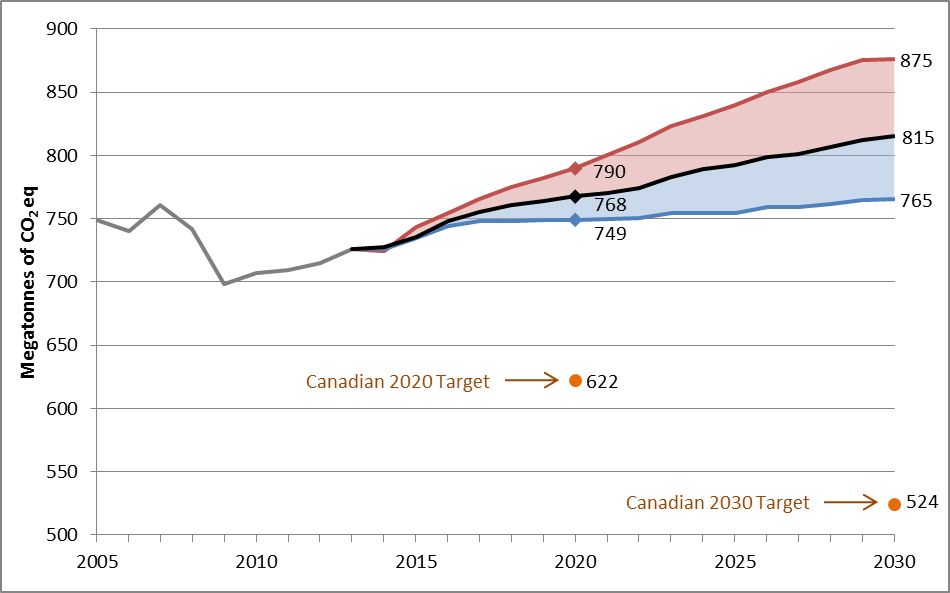
- The figure shows that Canada’s greenhouse gas emissions projections under a “with current measures” scenario are projected to be 768 megatonnes (Mt) CO2 eq in 2020 and 815 Mt CO2 eq in 2030. It also shows the expected range of the same projections under different economic and energy price and production scenarios. For 2020, the expected range of emissions could be between 749 Mt and 790 Mt. For 2030, the expected range of emissions could be between 765 Mt and 875 Mt. It must be noted that these projections do not include contributions for the land use, land-use change and forestry sector (LULUCF), as analysis of alternative accounting approaches remains ongoing. (Graph by Environment Canada)
IT SEEMS there’s never a law around when you need one.
I’m thinking of climate criminals, people who undermined climate change science for decades when they knew it was valid and were well aware that ignoring it meant human catastrophe. They’re getting away with murder. (Climate criminals do not include the ignorant. Ignorance is not a crime.)
But what about people like Rex Tillerson, the former chief executive officer of ExxonMobil and U.S. secretary of state?
Exxon was the corporate Joseph Goebbels of the losing war against climate change, sowing confusion and doubt about climate science. Doubly damning, the company did so despite research, from its own scientists, going back to 1977 about the reality and deadly implications of climate change.
Tillerson began his career with Exxon in 1975 and quickly rose to the company’s upper ranks. He cannot pretend he didn’t know about the vile propaganda his company was spreading or that he couldn’t have done something about it.
I like to think a Canadian criminal court could jail Tillerson under Section 219 of the Criminal Code:
Criminal negligence
219 (1) Every one is criminally negligent who
(a) in doing anything, or
(b) in omitting to do anything that it is his duty to do,
shows wanton or reckless disregard for the lives or safety of other persons. (Emphasis added.)
The maximum sentence when lives are lost is life in prison .

It’s reasonable to argue that Tillerson’s collaboration in a disinformation campaign against climate change science shows a “wanton disregard for the lives or safety of others”.
On the other hand, you could argue that investigating one of the world’s 10 largest companies is too much of an undertaking for our tiny country. However, much of the groundwork has already been done by U.S. states on behalf of Exxon shareholders. They’re arguing in civil court that shareholders weren’t properly advised of the threat to the value of their holdings posed by climate change.
Here, courtesy of the Pulitzer Prize-winning Inside Climate News is an overview of legal actions against Exxon in the U.S.
I’m certain the plaintiffs would gladly share their evidence against Exxon with Canadian investigators and I would like to see similar lawsuits here, but I’m far more concerned about the well-crafted public deception that undermined the fight against climate change.
Scientific American says “One thing is certain: in June 1988, when NASA scientist James Hansen told a congressional hearing that the planet was already warming, Exxon remained publicly convinced that the science was still controversial. Furthermore, experts agree that Exxon became a leader in campaigns of confusion. By 1989 the company had helped create the Global Climate Coalition (disbanded in 2002) to question the scientific basis for concern about climate change. It also helped to prevent the U.S. in 1998 from signing the international treaty, known as the Kyoto Protocol, to control greenhouse gases. Exxon’s tactic not only worked on the U.S. but also stopped other countries, such as China and India, from signing the treaty.” (Emphasis added.)
Remember, Exxon did this while possessing its own research validating climate change science.
So, I would like to see criminal charges under Section 219 and extradition requests to the U.S. for Tillerson and other Exxon executives.
But let’s not stop there. My guess is there are hundreds of equally guilty Canadians working for Exxon or other fossil fuel companies. As noted, the U.S. has done the groundwork, so let’s use it to hunt down our own climate criminals.
I understand that lawyers would probably shoot down this idea down because of some legal subtlety.
OK fine. Then we need a new law to instill palpable fear in Canada’s executive suites about degrading the environment. For example, executives inclined to secretly pollute so much as a trickling stream should be prepared for jail.
The environment is not an abstract concept: it’s our habitat. We are not trying to save the planet, which has survived climate change before; we are desperately trying to save ourselves.
People who get in the way belong behind bars. If our current laws can’t do the job, then let’s write new ones.
-30-